Saturday, December 21, 2013
Life long learning
Congratulations to Eden Prairie Physical Therapist, Meredith Butulis, on completing her MBA this weekend. This life-long learner also holds a Doctorate and Master's in Physical Therapy, Bachelor's in Pre-Med Health Studies, and several Personal Training and Pilates certifications.
Hip post op labral tear
After surgery, people typically ask how long it will take to get back to various activities. Today, we will focus on post-op hip labral repairs with bony resections.
A labral tear means that the cartilage rim that helps support your hip stability has been injured. Not all labral tears require surgery. Surgical procedures and post-op protocols are also highly variable. The ideas presented here relate to one of our more common protocols, but again, it does vary by surgeon and exact procedure.

Here are the typical time frames for common activities:
1 week: Driving (for left hip surgeries)
3 weeks: Walking without crutches, Driving for right hip surgeries
6 weeks: Elliptical trainer
10 weeks: Some jogging and sport training
12-16 weeks: Modified return to sport
6 months-1 year: High level competitive sport without restriction
We hope this provides you an overview of activities. You should always check with your surgeon on his/her specific time frames for your specific surgery. Have a question or idea to share? Leave us a post!
A labral tear means that the cartilage rim that helps support your hip stability has been injured. Not all labral tears require surgery. Surgical procedures and post-op protocols are also highly variable. The ideas presented here relate to one of our more common protocols, but again, it does vary by surgeon and exact procedure.
Here are the typical time frames for common activities:
1 week: Driving (for left hip surgeries)
3 weeks: Walking without crutches, Driving for right hip surgeries
6 weeks: Elliptical trainer
10 weeks: Some jogging and sport training
12-16 weeks: Modified return to sport
6 months-1 year: High level competitive sport without restriction
We hope this provides you an overview of activities. You should always check with your surgeon on his/her specific time frames for your specific surgery. Have a question or idea to share? Leave us a post!
Saturday, December 14, 2013
Patellofemoral syndrome
What is patellofemoral syndrome? This is a question that we hear quite often at OSR Physical Therapy!
Patellofemoral syndrome means that your kneecap is not staying in line with thigh when you perform activities like walking, stair climbing, running, squatting, lunging, and jumping.

Think of your kneecap (aka patella) like a train. Think of your thigh (aka femur) like a set of railroad tracks. The train needs to stay centered on the tracks while you perform activities.
While traditional physical therapy focuses on strengthening your VMO (aka vastus medialis) and providing orthotics (shoe inserts), we use a more comprehensive sports medicine approach at OSR.

As suggested at the annual Cincinnati Sport Medicine Conference, the focus needs to be on the hip, not so much at the knee cap. Therefore, we assess the hip, knee, ankle, foot, and even core for muscle imbalances. Once we find those imbalances, we create a comprehensive custom treatment plan to resolve the muscle imbalances and retrain how you are performing the activities that were provoking the pain.
Most of the time, we find that we focus much more on how the "train track" works, and then the "train" just needs a little fine tuning so you can enjoy activities again!
Here is a video of one "train track alignment" exercise that we find almost everyone benefits from at some point in time:
Have questions or comments? Leave us a post!
This article was written by Meredith Butulis, DPT, who works at our Eden Prairie office.
Patellofemoral syndrome means that your kneecap is not staying in line with thigh when you perform activities like walking, stair climbing, running, squatting, lunging, and jumping.

Think of your kneecap (aka patella) like a train. Think of your thigh (aka femur) like a set of railroad tracks. The train needs to stay centered on the tracks while you perform activities.
While traditional physical therapy focuses on strengthening your VMO (aka vastus medialis) and providing orthotics (shoe inserts), we use a more comprehensive sports medicine approach at OSR.

As suggested at the annual Cincinnati Sport Medicine Conference, the focus needs to be on the hip, not so much at the knee cap. Therefore, we assess the hip, knee, ankle, foot, and even core for muscle imbalances. Once we find those imbalances, we create a comprehensive custom treatment plan to resolve the muscle imbalances and retrain how you are performing the activities that were provoking the pain.
Most of the time, we find that we focus much more on how the "train track" works, and then the "train" just needs a little fine tuning so you can enjoy activities again!
Here is a video of one "train track alignment" exercise that we find almost everyone benefits from at some point in time:
Have questions or comments? Leave us a post!
This article was written by Meredith Butulis, DPT, who works at our Eden Prairie office.
Saturday, November 9, 2013
Anterior oblique system
Last week, we discussed the posterior oblique muscle system. This week, let's move on to the anterior oblique system. When your external obliques and opposite side adductor work together, you can create power. This is especially beneficial in throwing sports.

After you've activated any under-active muscles or reach the final stages of your rehab program, here are some conditioning exercises you may wish to consider to build the strength of your anterior oblique system:




After you've activated any under-active muscles or reach the final stages of your rehab program, here are some conditioning exercises you may wish to consider to build the strength of your anterior oblique system:

Saturday, November 2, 2013
Posterior Oblique Muscles and Exercises
Have you ever rehabbed a back, hip, knee, or ankle injury? If you rehabbed with a Physical Therapist at OSR, you likely incorporated some exercises for your glutes. Numerous Physical Therapy and Athletic Training research articles guide us in ensuring that we assess and treat hip weaknesses with any lower body injury.
At some point you will be ready to move beyond basic exercises. At this point, you might wonder, what comes after the basics like clams and bridges? Transitioning from the basics of Physical Therapy back into fitness and total body training in a logical progression is advised to achieve optimal performance.
Muscles not only work in isolation, but also in groups. These groups are referred to as muscle systems (aka subsystems or slings). This article will focus on the posterior oblique system. This refers to how your lats and gluteus maximus work together during every day motion and sports motion.

Here are three exercises that can be used to target how these muscle groups work together:
Squat to row: This can be done with a TRX, cable, or band. It can be progressed to standing on one foot instead of two.

Bridge lat pull: This is traditionally a Pilates exercise, but can be done with a band anchored to a fixed object.

Single leg RDL: This can be performed without weight, and then progressed to using dumbbells or kettlebells.

This article was written by Meredith Butulis, DPT, ACSM HFS, NASM CPT. Meredith is a Physical Therapist at our Eden Prairie location. OSR Physical Therapy does run an Aftercare program to transition from Physical Therapy back to sport.
At some point you will be ready to move beyond basic exercises. At this point, you might wonder, what comes after the basics like clams and bridges? Transitioning from the basics of Physical Therapy back into fitness and total body training in a logical progression is advised to achieve optimal performance.
Muscles not only work in isolation, but also in groups. These groups are referred to as muscle systems (aka subsystems or slings). This article will focus on the posterior oblique system. This refers to how your lats and gluteus maximus work together during every day motion and sports motion.

Here are three exercises that can be used to target how these muscle groups work together:
Squat to row: This can be done with a TRX, cable, or band. It can be progressed to standing on one foot instead of two.

Bridge lat pull: This is traditionally a Pilates exercise, but can be done with a band anchored to a fixed object.

Single leg RDL: This can be performed without weight, and then progressed to using dumbbells or kettlebells.

This article was written by Meredith Butulis, DPT, ACSM HFS, NASM CPT. Meredith is a Physical Therapist at our Eden Prairie location. OSR Physical Therapy does run an Aftercare program to transition from Physical Therapy back to sport.
Wednesday, October 16, 2013
Physical Therapy Month
October is Physical Therapy month. Have you ever wondered what kind of educational background Physical Therapists have? Check out this article on the basics of
Physical Therapists.
Have a question about becoming a Physical Therapist, or about the background or specialties of your specific Physical Therapist? Leave us a post!
Have a question about becoming a Physical Therapist, or about the background or specialties of your specific Physical Therapist? Leave us a post!
Monday, October 14, 2013
Introducing Minnetonka Athletic Trainer Kristin Kutch
I’m new to the Twin Cities and am very glad to have found a
home with OSR Physical Therapy. I moved to Twin Cities in July from Kansas City
due to a work move for my husband.
 Back in Kansas City I worked two years as the Head Athletic
Trainer for a high school in Independence, Missouri. I was solely responsible
for care of all athletes involved with the school’s 13 different sports. In
addition to working at the high school I also worked as an Athletic Trainer
with a youth hockey league, summer soccer league, and was part of the medical
staff for the 2013 NAIA Division I Basketball Tournament. I was also fortunate
enough to work as part of the stretcher crew for several professional soccer games
at Sporting Kansas City Stadium.
Back in Kansas City I worked two years as the Head Athletic
Trainer for a high school in Independence, Missouri. I was solely responsible
for care of all athletes involved with the school’s 13 different sports. In
addition to working at the high school I also worked as an Athletic Trainer
with a youth hockey league, summer soccer league, and was part of the medical
staff for the 2013 NAIA Division I Basketball Tournament. I was also fortunate
enough to work as part of the stretcher crew for several professional soccer games
at Sporting Kansas City Stadium.
I look forward to learning a lot in my new position at OSR
as well as offering my knowledge and experience of sport performance
enhancement. It is very rewarding as a clinician to see your patients return to
their sport or activity at their full capacity, something I look forward to
working towards every day at OSR.
Kristin is located at our Minnetonka office and works as a team with Physical Therapist, Matt Gannott.
Sunday, October 13, 2013
Introducing Eden Prairie Physical Therapist Meaghan Cox
Meet one of OSR's new providers: Meaghan Cox!

"I am very excited to be a new member of OSR working at the Eden Prairie clinic. I am originally from Regina, Saskatchewan, Canada where I grew up very involved in sports such as swimming, track and field, figure skating, Ukrainian dancing and watching a lot of hockey. However, artistic gymnastics was always my passion and I was grateful to be able to travel all over the country to compete at the Elite and National level. When I was 18, I moved to Illinois to attend college on a full gymnastics scholarship at Illinois State University. I also spent 1 year involved in my school’s acrobatic circus. After graduating with my Bachelor’s degree, I moved to Kentucky where I graduated with my Doctorate in Physical Therapy from The University of Kentucky.
While spending many hours in the gym, I sustained multiple injuries and spent my fair share of time in physical therapy. It was through this personal experience that I fell in love with the profession of physical therapy and knew that I wanted to spend my career helping athletes and active individuals get back to their respected sports and activities just as someone had done for me for so many years.
I plan to be active in the gymnastics population as well as high school and community events as I become settled into the Eden Prairie clinic. I also have a great interest in all sport and orthopedic injuries and look forward to working with all people to help them achieve their PT goals."
"I am very excited to be a new member of OSR working at the Eden Prairie clinic. I am originally from Regina, Saskatchewan, Canada where I grew up very involved in sports such as swimming, track and field, figure skating, Ukrainian dancing and watching a lot of hockey. However, artistic gymnastics was always my passion and I was grateful to be able to travel all over the country to compete at the Elite and National level. When I was 18, I moved to Illinois to attend college on a full gymnastics scholarship at Illinois State University. I also spent 1 year involved in my school’s acrobatic circus. After graduating with my Bachelor’s degree, I moved to Kentucky where I graduated with my Doctorate in Physical Therapy from The University of Kentucky.
While spending many hours in the gym, I sustained multiple injuries and spent my fair share of time in physical therapy. It was through this personal experience that I fell in love with the profession of physical therapy and knew that I wanted to spend my career helping athletes and active individuals get back to their respected sports and activities just as someone had done for me for so many years.
I plan to be active in the gymnastics population as well as high school and community events as I become settled into the Eden Prairie clinic. I also have a great interest in all sport and orthopedic injuries and look forward to working with all people to help them achieve their PT goals."
Focus on Women's Health: ACL and knee injury prevention exercises
Interested in understanding why females are more susceptible to knee injury? Would you like some exercises to include in your workouts that can help as part of your injury prevention plan?
See this National Academy of Sports Medicine article, written by Meredith Butulis, DPT. Meredith works out of our Eden Prairie office. Here is one of the sets of exercises you will find in the article:

See this National Academy of Sports Medicine article, written by Meredith Butulis, DPT. Meredith works out of our Eden Prairie office. Here is one of the sets of exercises you will find in the article:
Tuesday, September 10, 2013
Physical Therapy for Prehab before ACL reconstruction?
“Should I really go
to physical therapy for ‘prehab’ before I have my ACL reconstruction?”
This is a very common question asked by athletes who have
recently suffered an ACL tear, and the answer is YES. The single largest mistake people make is neglecting
the importance of regaining functional knee range of motion, maximizing
strength/coordination, and reducing swelling as much as possible BEFORE going
in for surgery. The pain and swelling caused
by inflammation after an ACL tear can produce reflex weakening of the muscles
surrounding the injured area. Neuromuscular control needs to be restored prior
to surgery in order to facilitate normal muscle recovery post-operatively. The
stronger the muscles are going in, the faster they will recover afterwards. Doing nothing for even the couple weeks
leading up to surgery can make your post-operative recovery much more
difficult.
In addition to the physical benefits of pre-operative therapy,
establishing a relationship with your Physical Therapist beforehand will
provide a huge mental boost and allow you to become prepared for surgery and
what is to be expected afterwards. An
ACL tear is a HUGE deal to an athlete and is a very difficult injury to come
back from mentally. Going into surgery
with a strong sense of mental preparedness enables the athlete to be both
confident and realistic about the rehab process and goal setting. Athletes are often nervous about surgery and
will likely forget to ask the surgeon the right questions. Working with your physical therapist before
allows the procedure to be explained thoroughly and gives the athlete/therapist
opportunity to discuss their rehabilitation program in detail, so that they
fully understand what is expected of them.
At OSR Physical Therapy, we specialize in the treatment of
athletic injuries and have had the opportunity to return many local athletes to
their sport in PRIME CONDITION following ACL Reconstruction. We are proud to be the choice provider for
many of our local high school athletes and are confident in our staff and
state-of-the art equipment. Please do
not hesitate to contact us to answer any questions you may have about ACL
Reconstruction and rehabilitation.
Here are some related links of interest:
http://www.nlm.nih.gov/medlineplus/ency/article/001074.htm
This article was created by Josh Rolfes, DPT. Josh works out of our Eden Prairie office.
This article was created by Josh Rolfes, DPT. Josh works out of our Eden Prairie office.
Thursday, August 22, 2013
Swimmer's shoulder
The start of fall sports season has begun filling OSR with high school sports injuries. This post will cover a common injury in swimmers : Swimmer’s shoulder.
Historically swimmer’s shoulder has been any pain in, or around the shoulder of a competitive swimmer. Specifically it is a type of impingement of the tendons of the rotator cuff muscles as they pass over the ball of the shoulder joint. Unlike “standard” impingement, swimmer shoulder is much more commonly associated with too much mobility in the shoulder joint as well as the shoulder blade.
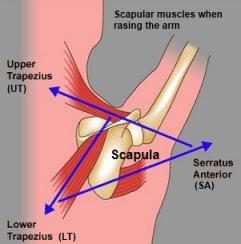
Due to the propulsion required by the upper body with all swim strokes, swimmers often demonstrate a stereotypically rounded, or forward shoulder posture. This posture is a result of weakness of the muscles that stabilize the shoulder blade (trapezius and rhomboids) as well as the rotator cuff, along with the strength of the muscles across the front of the shoulder (pectoralis and latissimus) that are required to move the swimmer through the water.

The resulting imbalance leads to a shoulder that does not have enough space on the top of the ball and socket joint to allow the tendons of the rotator cuff to pass without “pinching”, also known as shoulder impingement.

A swimmer with shoulder impingement must balance the need for an extremely mobile shoulder with enough strength in the scapular stabilizers and rotator cuff to prevent impingement. The best exercise to stabilize the shoulder blade is horizontal abduction, and the best to keep the rotator cuff group strong is sidelying external rotation. The following are pictures and brief descriptions of each.
Horizontal Abduction: Lie on your stomach with the arm hanging down off the edge of the bed or table. Start the motion by squeezing your shoulder blade in toward your spine and then raise your arm out to the side as if to make the letter “T”. Slowly return to the starting position.
Sidelying External Rotation: Lie on your side with the arm you want to exercise facing up. Place a small towel roll between your elbow and ribs. With the elbow bent to 90 degrees, slowly raise the forearm toward the ceiling then slowly return.
Both exercises should be performed with low weights (0-3 lbs) for high repetitions (30-50) every other day. These exercises should NOT be painful, but fatigue and muscle “burn” can be expected. Relative rest from your daily yardage while the pain persists is also recommended.
If your shoulder pain continues with the combination of these exercises and relative rest, contact your physician or call any of our offices with questions or to sign up for a free injury consultation with one of our certified athletic trainers.
This article was created by Ryan Koepp, DPT with collaboration of Andrew Ernst, ATR. This team works out of our Eden Prairie office.
Historically swimmer’s shoulder has been any pain in, or around the shoulder of a competitive swimmer. Specifically it is a type of impingement of the tendons of the rotator cuff muscles as they pass over the ball of the shoulder joint. Unlike “standard” impingement, swimmer shoulder is much more commonly associated with too much mobility in the shoulder joint as well as the shoulder blade.
Due to the propulsion required by the upper body with all swim strokes, swimmers often demonstrate a stereotypically rounded, or forward shoulder posture. This posture is a result of weakness of the muscles that stabilize the shoulder blade (trapezius and rhomboids) as well as the rotator cuff, along with the strength of the muscles across the front of the shoulder (pectoralis and latissimus) that are required to move the swimmer through the water.

The resulting imbalance leads to a shoulder that does not have enough space on the top of the ball and socket joint to allow the tendons of the rotator cuff to pass without “pinching”, also known as shoulder impingement.
A swimmer with shoulder impingement must balance the need for an extremely mobile shoulder with enough strength in the scapular stabilizers and rotator cuff to prevent impingement. The best exercise to stabilize the shoulder blade is horizontal abduction, and the best to keep the rotator cuff group strong is sidelying external rotation. The following are pictures and brief descriptions of each.
Horizontal Abduction: Lie on your stomach with the arm hanging down off the edge of the bed or table. Start the motion by squeezing your shoulder blade in toward your spine and then raise your arm out to the side as if to make the letter “T”. Slowly return to the starting position.
Sidelying External Rotation: Lie on your side with the arm you want to exercise facing up. Place a small towel roll between your elbow and ribs. With the elbow bent to 90 degrees, slowly raise the forearm toward the ceiling then slowly return.
Both exercises should be performed with low weights (0-3 lbs) for high repetitions (30-50) every other day. These exercises should NOT be painful, but fatigue and muscle “burn” can be expected. Relative rest from your daily yardage while the pain persists is also recommended.
If your shoulder pain continues with the combination of these exercises and relative rest, contact your physician or call any of our offices with questions or to sign up for a free injury consultation with one of our certified athletic trainers.
This article was created by Ryan Koepp, DPT with collaboration of Andrew Ernst, ATR. This team works out of our Eden Prairie office.
Friday, August 16, 2013
Minnetonka clinic is now open!

You can schedule with Physical Therapists, Rusty Wallman and Matt Gannott, at this location. We continue to operate our Chanhassen and Eden Prairie clinics as well.
Friday, August 9, 2013
Thigh injuries and water sports
This month, I have seen a remarkably high number of thigh contusions/injuries from people coming into contact with boating docks during water sports.

If you find yourself with a serious thigh bruise after this incident, or after a sports injury, here are a few recommendations:
1. Get the injury evaluated by a medical professional to ensure that you have not injured your underlying bone.
2. Ice --15 min on. 15 min off
3. Compress--Using an elastic bandage can help control swelling
4. For the first 24 hours, try to keep your knee in a bent position
You can find more technical and detailed information on management via this link.
If you find yourself with a serious thigh bruise after this incident, or after a sports injury, here are a few recommendations:
1. Get the injury evaluated by a medical professional to ensure that you have not injured your underlying bone.
2. Ice --15 min on. 15 min off
3. Compress--Using an elastic bandage can help control swelling
4. For the first 24 hours, try to keep your knee in a bent position
You can find more technical and detailed information on management via this link.
Wednesday, July 31, 2013

Monday, July 29, 2013
Patellofemoral Pain
"The front of my knees hurt when I sit, when I go up stairs, when I do squats" . . . does this sound like you or someone you know? This is a very common symptom that Physical Therapists at OSR assess and treat. Many times this is due to patellofemoral syndrome or kneecap tracking problems.

This affects kids, teens, and adults. It is not uncommon to see someone who has had this complaint for many years, although treating it when it first becomes a problem leads to a much faster resolution.
Check out this WebMD article, which explains the basics of this condition. Physical Therapists perform an assessment and then progress exercises in supervised therapy over several weeks to ensure that you reach your goals in a safe and effective manner.
This affects kids, teens, and adults. It is not uncommon to see someone who has had this complaint for many years, although treating it when it first becomes a problem leads to a much faster resolution.
Check out this WebMD article, which explains the basics of this condition. Physical Therapists perform an assessment and then progress exercises in supervised therapy over several weeks to ensure that you reach your goals in a safe and effective manner.
Sunday, July 21, 2013
Patellofemoral pain, ACL tears, back pain, pronation distortion and more
Knee pain, Achilles pain, torn ACLs, back pain . . .the list goes on and on! Many times these injuries increase in the summer, and sometimes this is due to changing footwear from more supportive arches to flip flops.
However, the solution often isn't just in the shoes. Many people also have pronation distortion syndrome, which can contribute to pain and injury. The good news is that it can be improved with exercises!
Check out this National Academy of Sports Medicine article for lots of assessments and exercises to help with your injury prevention workouts!
However, the solution often isn't just in the shoes. Many people also have pronation distortion syndrome, which can contribute to pain and injury. The good news is that it can be improved with exercises!
Check out this National Academy of Sports Medicine article for lots of assessments and exercises to help with your injury prevention workouts!
Saturday, July 13, 2013
New clinic opens this week!
OSR opens the doors to it's Minnetonka clinic this week! You will find it right across from the Minnetonka High School. For scheduling or questions call 952-512-2400. You can schedule with our Minnetonka Physical Therapists, Rusty Wallman and Matt Gannot, as well as their Athletic Training care team!

Wednesday, July 3, 2013
Athletic Training Job Opening
OSR Physical Therapy has a new opening for an Athletic Trainer. Athletic Trainers at OSR work in a clinic setting in direct patient care, as well as performing outreach. If you are interested, please send your résumé to Nate Tellers at nate.tellers@osrpt.com.
Saturday, June 22, 2013
Baseball injuries part 3
Welcome to the final article in our baseball series for the month of June!
The third common throwing injury is a condition called
scapular dyskinesis. This occurs when the shoulder blade is not moving fluidly
with the arm. Without our shoulder blade moving, we can reach just above
shoulder height. The movement of the arm and shoulder blade together is what
allows us to reach above our head. If this ‘rhythm’ is not in sync, it can
cause defects in a thrower’s mechanics and also cause impingement in the joint as
a thrower tries to force them into the correct arm slot.
Finally, the most preventable throwing injury is caused by
overuse. Often pitchers get themselves in trouble when they fail to rest in
between starts. By throwing with fatigued muscles a player is at risk of
decreased shoulder stabilization which can cause injury to both their shoulder
and elbow. It is imperative that a pitcher fully recovers before making the
subsequent start.If you notice a loss of speed or distance, this is a sign of fatigue.
Baseball season is enjoyable for players, coaches, parents
and fans. By keeping the shoulder and elbow strong and pain free that enjoyment
will last the whole summer. Have questions? Leave us a post!
Subscribe to:
Posts (Atom)